Dermal Filler vs Skin Booster: Key Differences for Aesthetics Clinics
In contemporary aesthetic medicine, successful facial rejuvenation increasingly depends on a precise understanding of both structural support and skin quality. Patients rarely present with isolated volume loss or isolated dehydration; most exhibit a combination. Mastering the difference between filler and skin booster enables practitioners to select the right tool or combination for each individual, optimising outcomes while managing expectations and minimising risk.At the heart of this distinction lies the science of hyaluronic acid (HA) and how its molecular architecture is engineered: crosslinked versus noncrosslinked (or hybrid stabilised) forms. This foundational difference in rheology, degradation profile, and biological behaviour drives everything from injection technique and depth to clinical indication, longevity, and patient selection.
The Foundational Science: Crosslinked vs Noncrosslinked Hyaluronic Acid
Native HA in the dermis is a linear, noncrosslinked glycosaminoglycan that binds up to 1000 times its weight in water and participates in cell signalling via CD44 receptors. In its natural state it turns over rapidly (half life of hours to days).
To create dermal fillers, manufacturers introduce chemical crosslinkers (commonly BDDE) that form covalent bonds between HA chains. This produces a three dimensional gel network with significantly higher elastic modulus (G prime) and resistance to enzymatic degradation by hyaluronidases. The result is a product that maintains structural integrity, provides lift and volume where placed, and persists for 6 to 18 months or longer depending on degree of crosslinking, concentration, and injection plane.
Skin boosters, by contrast, typically employ noncrosslinked high molecular weight HA or specially stabilised hybrid complexes (for example Profhilo NAHYCO technology combining high and low MW HA without chemical crosslinkers). These remain fluid, spread readily through the extracellular matrix, and deliver intense, diffuse hydration. While their physical presence is shorter (often 2 to 4 weeks), the biological effects (fibroblast stimulation, improved collagen and elastin organisation, and enhanced skin quality) can persist for months.
A 2023 study by Duteil et al. demonstrated that intradermal noncrosslinked HA significantly improved hydration, firmness, radiance, and fine wrinkles, while crosslinked formulations are engineered for mechanical volumisation rather than widespread biorevitalisation. Rheological analyses further confirm that noncrosslinked or hybrid products exhibit distinct viscoelastic behaviour under mechanical stress, making them better suited to superficial dermal placement and uniform distribution.
Mechanism of Action and Clinical Indications
Dermal fillers act primarily through mechanical displacement and support. They are indicated for volume restoration, contour definition, and correction of moderate to severe folds and deficits (for example cheeks, chin, jawline, temples, and nasolabial folds). They excel when the primary complaint is structural (hollowing, sagging contours, or deep static lines caused by fat pad atrophy or bone resorption).
Skin boosters function through biorevitalisation. High concentrations of HA (typically 20 to 32 mg per mL) attract and retain water while the material and its degradation fragments stimulate fibroblasts, improve extracellular matrix quality, and enhance skin elasticity, texture, and luminosity. They are ideal for photoaged, dehydrated, crepey, or dull skin; fine lines; and overall skin quality improvement. They are particularly valuable in younger patients seeking prejuvenation or glass skin effects, and in maintenance regimens for mature skin.
A 2024 review by Yi et al. highlights how skin boosters evolved from repurposed fillers into a distinct category targeting dermal health beyond simple volumisation. Randomised data even suggest advantages over traditional fillers for certain texture concerns, such as atrophic acne scars.
Treatment Protocols, Longevity, and Patient Selection
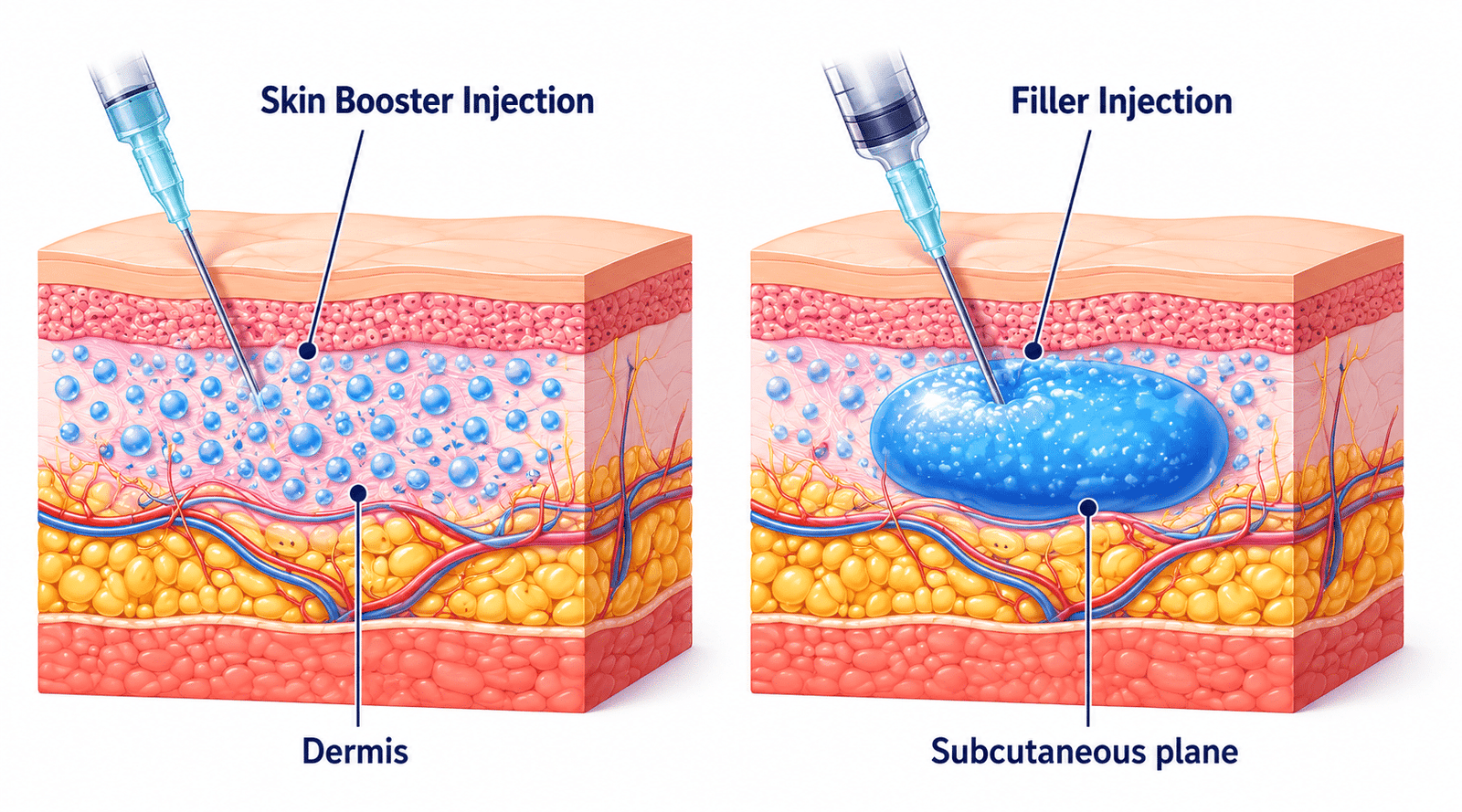
Injection technique differs markedly. Crosslinked fillers are placed with precision, often using cannula in the deep dermis, supraperiosteal plane, or fat compartments, to achieve lift and avoid superficial irregularities. Over correction or superficial placement risks Tyndall effect or nodules.
Skin boosters are delivered via multiple micro injections or specific point techniques (for example Profhilo Bio Aesthetic Points, 5 points per side of the face) into the superficial to mid dermis or subdermal layer. The goal is even distribution rather than localised volume. Most protocols involve an initial course of two to three sessions spaced three to four weeks apart, followed by maintenance every four to six months.
Longevity also diverges. Volumising results from crosslinked fillers typically last from 9 to 18 months. Skin booster effects on hydration and quality often become apparent after the second session and can be maintained with periodic treatments; the biostimulatory benefits may outlast the physical presence of the HA.
Patient selection is key. A patient with significant mid face volume loss and deep nasolabial folds will benefit most from crosslinked HA filler. A patient with good underlying structure but dehydrated, textured, or crepey skin is better served by a skin booster (or a staged approach). Many patients benefit from combination therapy: structural support first, followed by skin quality optimisation.
Optimising Outcomes for Nasolabial Folds: Evidence for Crosslinked Dermal Fillers
For pronounced nasolabial folds, crosslinked HA fillers remain the evidence based cornerstone in UK and international practice. Systematic reviews and meta analyses of randomised trials demonstrate consistent, sustained improvement in Wrinkle Severity Rating Scale (WSRS) scores, with high patient and investigator satisfaction and low rates of serious adverse events when proper technique and product selection are used.
Popular, well studied options in UK clinics include members of the Juvederm and Restylane families, chosen according to rheology, cohesivity, and G prime to match the
anatomical requirements of the fold. Skin boosters can complement these results by improving surrounding skin quality and reducing the appearance of fine lines, but they do not replace the mechanical correction provided by appropriately selected crosslinked fillers.
Safety Profiles and Current 2026 Trends
Both modalities have excellent safety records when performed by trained practitioners using authentic products. Fillers carry a small risk of vascular compromise if placed intravascularly; skin boosters, being more superficial and fluid, have a lower risk of vascular events but require attention to even distribution to avoid transient lumps.
Current trends emphasise regenerative and holistic approaches: skin boosters are increasingly used for prejuvenation, combination protocols with energy based devices or polynucleotides, and body applications (neck, decolletage, hands). Hybrid technologies and multi molecular weight HA formulations continue to gain traction for their ability to deliver both hydration and mild remodelling without traditional crosslinkers.
Sourcing Quality Products for Consistent Clinical Results
UK aesthetics clinics that prioritise reproducible outcomes and patient safety naturally gravitate toward reputable aesthetics suppliers who maintain rigorous cold chain logistics, product authenticity, and regulatory compliance (MHRA or CE marked medical devices). Whether purchasing for immediate clinical use or exploring established wholesale channels for dermal fillers, the emphasis remains on traceability, practitioner training support, and products backed by robust clinical data.
What the Research Tells Us: Key References
Yi KH et al. (2024). Skin boosters: Definitions and varied classifications. PubMed https://pubmed.ncbi.nlm.nih.gov/38481069/ (PMC full text available).
Allen J et al. (2024). Current Knowledge and Regulatory Framework on the Use of Hyaluronic Acid Fillers and Skin Boosters. Cosmetics https://www.mdpi.com/2079-9284/11/2/54.
Duteil L et al. (2023). The Effects of a Noncrosslinked Hyaluronic Acid Gel on Facial Skin Quality. PMC https://pmc.ncbi.nlm.nih.gov/articles/PMC10005802/.
Systematic reviews on HA fillers for nasolabial folds (for example Stefura et al., 2021 and subsequent updates).
Multiple Profhilo and hybrid HA studies demonstrating bioremodelling effects on texture, elasticity, and laxity (Sparavigna, Cassuto et al.).
Frequently Asked Questions from Professional Aesthetics Communities
How do I decide between a traditional dermal filler and a skin booster (or Profhilo type product) when a patient has both mild volume loss and poor skin quality?
Assess the dominant concern first. Significant structural deficit or deep folds usually requires crosslinked filler for mechanical support. Skin quality issues (dehydration, texture, fine lines, crepiness) respond best to skin boosters. Many patients achieve optimal results with a staged or combination approach: structure first, then quality.
What are the main rheological and clinical differences between crosslinked HA fillers and noncrosslinked or hybrid skin boosters that affect treatment planning?
Crosslinked fillers have higher G prime and cohesivity; they resist deformation and provide localised volume. Noncrosslinked or hybrid boosters are more fluid, spread easily, and prioritise widespread hydration plus biological stimulation. This dictates depth (deeper for fillers, more superficial for boosters), technique, and expected effect profile.
Is there evidence or accepted protocols for combining dermal fillers and skin boosters?
Yes. Many practitioners stage treatments (filler first for structure, booster two to four weeks later for quality) or use them in different facial zones in the same session. Clinical data support improved overall outcomes when both volume and skin health are addressed.
For nasolabial fold correction, which crosslinked HA fillers have the strongest evidence base in UK relevant practice?
Well documented options from the Juvederm and Restylane ranges have extensive RCT and real world data showing sustained WSRS improvement and favourable safety. Product choice depends on fold depth, skin thickness, and desired lift versus integration.
What adverse events should practitioners monitor most closely with superficial skin boosters versus deeper fillers?
With boosters: transient oedema, bruising, or unevenness from superficial placement. With fillers: vascular compromise (rare but serious), nodules, or Tyndall effect if placed too
superficially. Both require thorough anatomical knowledge and, ideally, ultrasound guidance in higher risk areas.
How do longevity and maintenance schedules differ in real world practice?
Crosslinked fillers often deliver visible structural results for 9 to 18 months. Skin boosters typically require an initial course of two to three treatments; maintenance is commonly every four to six months to sustain hydration and quality improvements. Biostimulatory effects can extend perceived benefits beyond the presence of the material.
In 2026, regenerative aesthetics practice, how are leading UK clinics using skin boosters alongside traditional fillers?
Forward thinking clinics integrate boosters for overall skin health, prevention, and enhancement of filler outcomes. This structure plus quality philosophy improves patient satisfaction, natural appearance, and long term skin resilience.
By understanding these nuanced differences, rooted in the fundamental distinction between crosslinked and noncrosslinked hyaluronic acid technologies, practitioners can deliver more precise, evidence based, and satisfying results. The modern aesthetics clinic that masters both modalities positions itself at the forefront of patient centred, regenerative care.